Togo's HIV Gains Are Real. So Are Concerns About Emerging Drug Resistance.

(Togo First) - While Togo has achieved an 85% viral suppression rate among people living with HIV, the emergence of resistance to dolutegravir, the cornerstone drug in the fight against AIDS, raises concerns about the sustainability of these gains. In January 2025, CARESP released the first surveillance findings among young Togolese patients. Against a backdrop of declining international funding and the absence of any short-term therapeutic alternative, heightened vigilance is essential.
Researchers in Togo have found early signs of resistance to dolutegravir, the frontline HIV drug, among children and adolescents on treatment, even as the country records broad progress in controlling the epidemic.
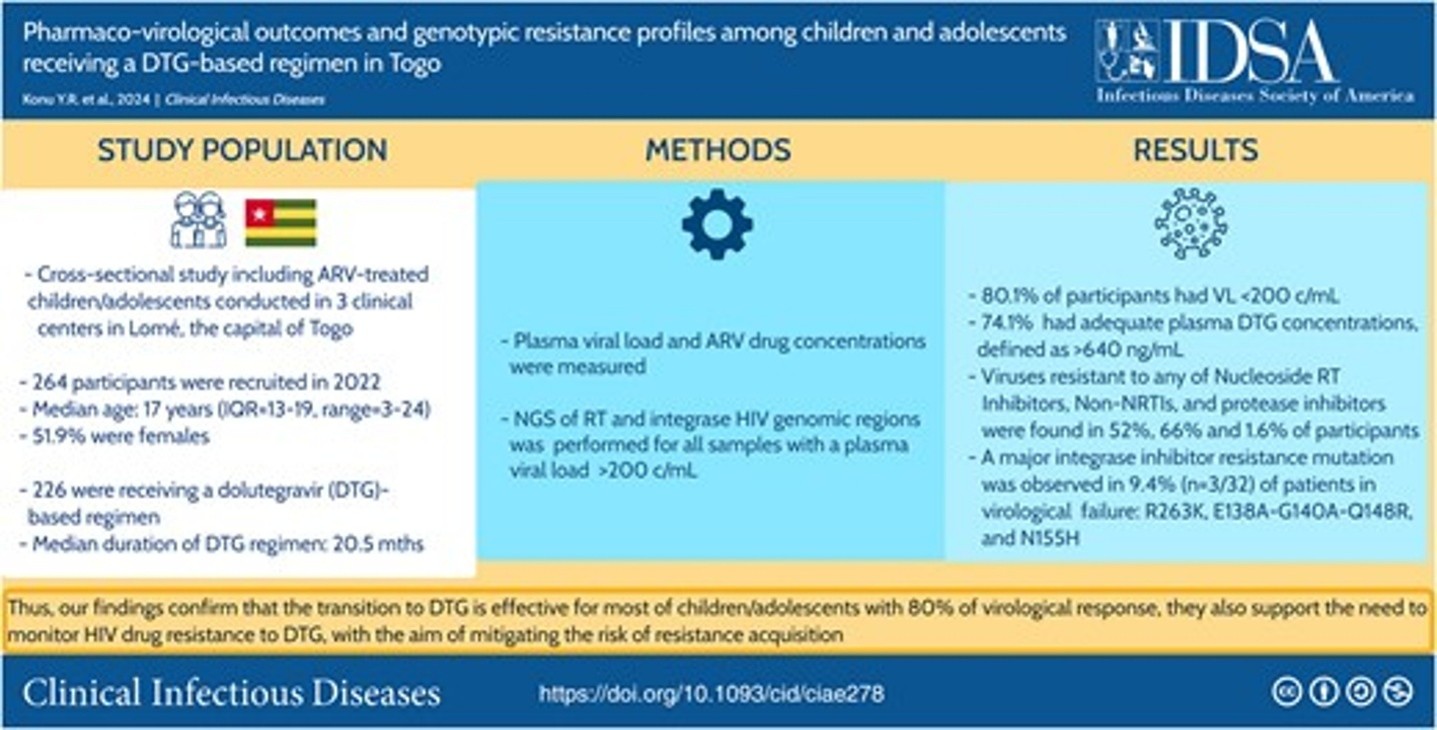
Scientists at the African Center for Research in Epidemiology and Public Health (CARESP), led by Professor Didier Koumavi Ekouevi, analyzed genetic data from HIV samples taken from 264 Togolese children and adolescents. The results, published in Clinical Infectious Diseases in January 2025, present a mixed picture: 80% of young patients on dolutegravir had undetectable viral loads, but nearly 10% of those experiencing virological failure showed signs of resistance to the drug, which is considered the latest-generation HIV treatment currently available.
"Dolutegravir is effective, and that is why we recommended switching all patients to this treatment," said Dr. Yao Rodion Konu, a medical epidemiologist and the study's lead author, who is a researcher at the University of Lomé and the University of Bordeaux. "But because everyone is now using this drug, we have an interest in staying vigilant. If this drug stops working, what alternatives will we have?"

In July 2019, the WHO recommended dolutegravir as the preferred option for all people living with HIV, including children and adolescents, citing its superior virological efficacy and high genetic barrier. Togo moved quickly: by 2020, dolutegravir had been integrated into first-, second- and third-line treatment. "By 2022, more than 95% of patients were on a dolutegravir-based regimen," Dr. Konu said. Of the 96,000 people living with HIV monitored in the country, around 10,000 are children and adolescents under 15. By end-2024, according to the National AIDS Council (CNLS), 92% of Togolese people living with HIV were on treatment and 85% had undetectable viral loads, compared with 84% and 76% respectively in 2023.
Togo has made significant strides against HIV over recent decades. Between 2023 and 2024, the share of people living with HIV who knew their status rose from 90% to 98%. Antiretroviral treatment coverage increased from 84% to 92%, and the viral suppression rate climbed from 76% to 85%. Coverage of programs to prevent mother-to-child transmission rose from 85% to 87%. The CNLS attributes these gains to sustained strategic and operational planning since 2005, which has strengthened the effectiveness of HIV programs and improved governance of the national response.
Against this backdrop, Professor Ekouevi, who leads CARESP's research on this issue, framed the emergence of resistance signals as part of the natural evolution of HIV treatment. "This is part of the normal treatment cycle. Treatment regimens are typically updated every ten years or so, depending on resistance levels. It is common, it is normal, it happens frequently," he said in an interview with Togo First.
Mutations to Monitor Among Young Patients
Between August and November 2022, researchers enrolled 264 participants aged 18 months to 24 years across three centers in Lomé, of whom 226 had been on dolutegravir for a median of 20.5 months. A first finding: 19.2% of participants had undetectable plasma concentrations of antiretrovirals, suggesting they were not taking their medication. "This is a major challenge among adolescents," Dr. Konu acknowledged. "The reasons include treatment fatigue, the challenges of adolescence, and limited support from parents or guardians."
More notable was what emerged among patients in virological failure. Of the 32 participants in virological failure for whom integrase sequencing could be performed, three had a major dolutegravir resistance mutation, a rate of 9.4%. "These three patients were receiving dolutegravir as a first-line treatment. None had prior exposure to raltegravir or received anti-tuberculosis treatment," the authors note. Two of them had adequate plasma concentrations, ruling out simple non-adherence as an explanation.
Prof. Didier Koumavi Ekouevi, physician-epidemiologist and president of the African Center for Research in Epidemiology and Public Health (CARESP).
Professor Ekouevi stressed the importance of reading these figures carefully. "When you look at 100 patients on treatment, you first identify those for whom treatment is not working. If 10% are failing, you need to know whether they are truly failing or simply non-adherent. We had 264 people, with resistance detected in three of them. Numbers need to be interpreted in context. We need to keep monitoring."
A Regional Phenomenon Under Closer Watch
Togo is not an isolated case. In March 2024, the WHO had already raised the alarm over the spread of dolutegravir resistance, with levels exceeding those seen in clinical trials, while noting the fragmentary nature of available data. The DTG RESIST study, published in May 2025 and covering 227 integrase sequences from seven African countries, returned more alarming findings: 26% of people in virological failure on dolutegravir had at least one major resistance mutation, and 21.6% showed high-level resistance. A Mozambican cohort published in September 2025 identified resistance in 46.4% of patients tested after confirmed failure. Togo's rate of 9.4% falls in an intermediate range, well below the most critical situations in southern Africa.
In its 2025 report on HIV drug resistance, the WHO noted that acquired resistance to dolutegravir could be more significant than anticipated, particularly among people who have received multiple prior treatments, while also noting that more than 90% of adherent patients achieve sustained viral suppression.
For Dr. Konu, the resistance is not solely attributable to the drug itself. "The WHO believes it is linked to how it is used in certain contexts, marked by delays in care and discontinuous treatments where adherence is not maintained," he said.
Zero Primary Resistance: A Confirmed Piece of Good News
In November 2025, a national CARESP and PNLS-HV-IST study of 321 treatment-naive Togolese adults newly diagnosed with HIV, published in Frontiers in Public Health, detected no major dolutegravir resistance mutations across a sample covering all six of the country's health regions. Professor Ekouevi said analyses conducted among patients who had not yet started treatment revealed no cases of primary resistance. "We found no cases, which is encouraging. Nevertheless, continued monitoring remains necessary," he said.

Dr. Rodion T. Konu, epidemiologist, biostatistician and research fellow at CARESP.
The same study did, however, identify accessory mutations associated with resistance to first-generation integrase inhibitors in 17.2% of samples, a signal that warrants monitoring over time.
Togolese Research With International Standing
The CARESP pediatric study relied on next-generation sequencing (Oxford Nanopore), which detected minority variants present at between 5% and 20% within the viral population. "These minority variants change the resistance interpretation for at least one antiretroviral in 10 out of 19 cases," Dr. Konu said. Conducted in partnership with the BIOLIM laboratory at the University of Lomé, the IAME unit at Paris Cité and the WHO office in Togo, the study also found high rates of resistance to older drug classes: 52% of viruses showed resistance to NRTIs and 66% to NNRTIs. "If dolutegravir loses its effectiveness and the other classes are already compromised, the alternatives become limited in a resource-constrained country like Togo," the researcher said.
To move beyond Lomé and a solely pediatric population, CARESP is conducting a national study funded by the Global Fund, at the request of the national HIV program. "We have 20 sites across the six health regions where we will collect samples and look at what is happening," Dr. Konu said, with the study targeting secondary resistance in people on treatment for at least one year. In May 2025, a delegation from ANRS, Inserm and IRD traveled to Lomé to launch the PRISME project, a partnership linking the CFRSP at the University of Lomé, directed by Professor Ekouevi, with Togolese health institutions.
Optimizing Resources, Monitoring Without Alarmism
Faced with resource constraints, Dr. Konu's team has developed an algorithm combining pharmacological results and viral load. "The idea is to avoid costly resistance testing on all patients in virological failure. Those with a detectable viral load but undetectable drug concentrations are probably non-adherent: no need for genotyping. Those with detectable drugs and a high viral load are the real candidates," he explained. Applied to the pediatric study, the algorithm would have reduced the number of genotypic tests needed by 64%. In France, Professor Ekouevi noted, treatment is never changed without individualized resistance testing comparable to antibiotic susceptibility testing, an approach that is out of reach in most low-income countries.

These advances sit within a broader positive national trend: HIV-related deaths fell 65% between 2010 and 2023, from 6,600 to 2,300. But these gains face threats. On December 1, 2024, Professor Vincent Pitche, coordinator of the CNLS permanent secretariat, warned of "a period of turbulence linked to the reduction of international funding." Togo relies heavily on the Global Fund to finance its HIV programs, in a sub-Saharan Africa that accounts for 67% of people living with HIV worldwide, approximately 25.6 million in 2023.
"The challenge is twofold," Dr. Konu said. "Maintaining the current level of care with declining resources, and investing in resistance surveillance to preserve the effectiveness of our tools."
Despite rising resistance signals, no change in the frontline molecule is being considered in the near term. "I do not think we will change before 2030. It takes time to accumulate data. A change has to happen because it has enormous economic implications, since we have only one drug for all patients," Professor Ekouevi said. "There is still not enough evidence to answer that question, which is why continuing research is important," Dr. Konu added, noting that the WHO itself had expressed similar reservations in 2024.
With 22 million people worldwide on dolutegravir-based treatment, monitoring resistance has become strategically important worldwide. "Our results confirm that this transition is effective for most individuals," Dr. Konu concluded, "but they also support the need to monitor dolutegravir resistance, with the goal of reducing the risk of resistance acquisition and subsequent transmission."
Ayi Renaud Dossavi

















